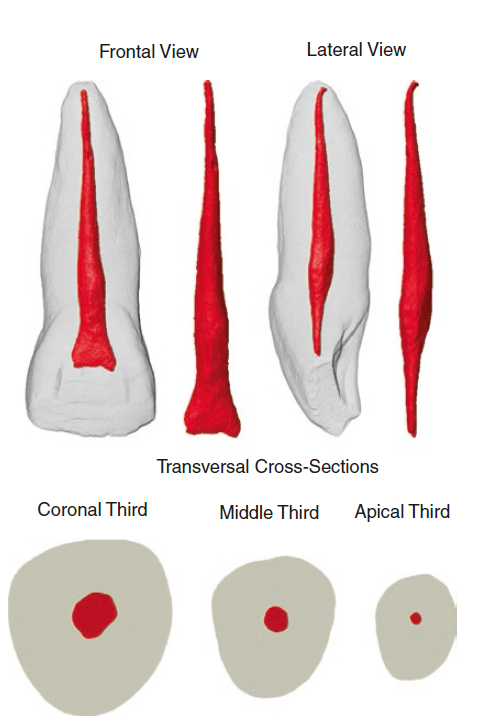
The root of the central incisor in the upper jaw is often thicker than the roots of the surrounding teeth. The shape of the cross-section of the root can vary and may be triangular, circular, or oval in shape. In mature teeth, the canal within the root tends to taper towards the tip of the tooth and may have slight curves near the apex.
The maxillary central incisors are centered in the maxilla, one on either side of the median line, with the mesial surface of each in contact with the mesial surface of the other. The pulp cavity follows the general outline of the crown and root. In this way, pulp chamber is very narrow in the incisal region and wider in the mesiodistal dimension than in the labiolingual dimension.
Morphological aspects of the root and root canal anatomy of maxillary central incisors
| Tooth notation (right/left) | (8 and 9), (1| and |1), or (#11 and #21) |
| Overall length | 23.6 mm (16.5–32.6 mm) |
| Root length | 13.0 mm (6.3–20.3 mm) |
| Complete root formation | 9.3–10.6 years (male-female) |
| Tooth axes angulation | 3–5° (orthoradial) and 15–20° (proximal) |
| Number of roots | 1 (100%)a 1 (99.94%), 2 (0.06%)b |
| Apical root curvature | Straight (75%), buccal (9.3%), distal (7.8%), mesial (4.3%), palatal (3.6%) |
| Root grooves | No prominent groove |
| Number of canals | 1 (100%)a 1 (99.2%), 2 (0.8%)b |
| Canal configuration | Type I (100%)a Types I (99.2%), IV (0.5%), II (0.1%), III (0.1%), and V (0.1%)b |
| Canal cross-section | Coronal, triangular with the mesial side longer than the distal side; middle, oval; apical, round |
| Canal taper | BL, 0.11 mm/mm; MD, 0.06 mm/mm |
| Transverse anastomosis | – |
| Furcation canals | – |
| Apical foramen position | Central, 12%; lateral, 88% |
| Accessory canals | 18.9–42.6% (coronal, 1%; middle, 6%; apical, 93%) |
| Apical ramification | 8.1–27.9% |
| Canal curvature | Clinical view, 0–26°; proximal view, 0–18° |
| Canal diameter | BL: 0.34 mm (0.15–0.69 mm) MD: 0.30 mm (0.14–0.59 mm) |
| Anomalies | Two canals [13–15]; three canals [16]; four canals [17]; two roots [13–15]; radicular groove [18]; fusion/gemination [19] |
| Clinical remarks | If a great amount of irritation-induced dentin is produced, pulp chamber may be partially or completely obliterated; a total of 79.7% of all foramina are located approximately 0.5 mm or less from the apex and 94.9% are approximately 1.0 mm or less away; 56.4% of the lateral canals have a mean diameter less than a size 10 K-file; lingual shoulder should be removed as it prevents direct access to the root canal, deflecting files and often resulting in ledge or perforation. In older patients, the roof of the pulp chamber is often first encountered in the region of the tooth cervix. For this reason, the access cavity must often be made near to the incisal edge to achieve the necessary straight-line access to the root canal |
The access cavity is initiated by penetrating the bur occlusal to the cingulum, avoiding the incisal edge. Once penetration to the root canal is achieved, the access cavity must be refined in a mesio-distal direction to remove the entire roof associated with the pulp horns. The access cavity achieves a roughly triangular shape with this preparation, which mirrors the anatomy of the pulp chamber