The maxillary lateral incisor complements the central incisor in terms of function and appearance. The two teeth have similar crowns, but the lateral incisor is smaller in size except for its root length. The pulp chamber of the lateral incisor is narrow near the incisal region of the tooth and becomes wider near the cervical level of the tooth. Additionally, the pulp horns of the lateral incisor are typically more pronounced.
Morphological aspects of the root and root canal anatomy of maxillary lateral incisors
| Tooth notation (right/left) | (7 and 10), (2| and |2), or (#12 and #22) |
| Overall length | 22.5 mm (17.7–28.9 mm) |
| Root length | 13.4 mm (9.6–19.4 mm) |
| Complete root formation | 9.7–11.1 years (male-female) |
| Tooth axes angulation | 5–6° (orthoradial) and 17–20° (proximal) |
| Number of roots | 1 (100%) 1 (99.94%) 2 (0.06%) |
| Apical root curvature | Distal (49.2%), straight (29.7%), palatal (3.9%), buccal (3.9%), mesial (3.1%), S-shaped (1.6%), others (8.6%) |
| Root grooves | Shallow depression on the middle of mesial root surface |
| Number of canals | 1 (97%), 2 (3%) 1 (98.5%), 2 (1.5%) |
| Canal configuration | Type I (100%)a Types I (98.5%), II (0.8%), V (0.4%), III (0.2%), IV (0.1%)b |
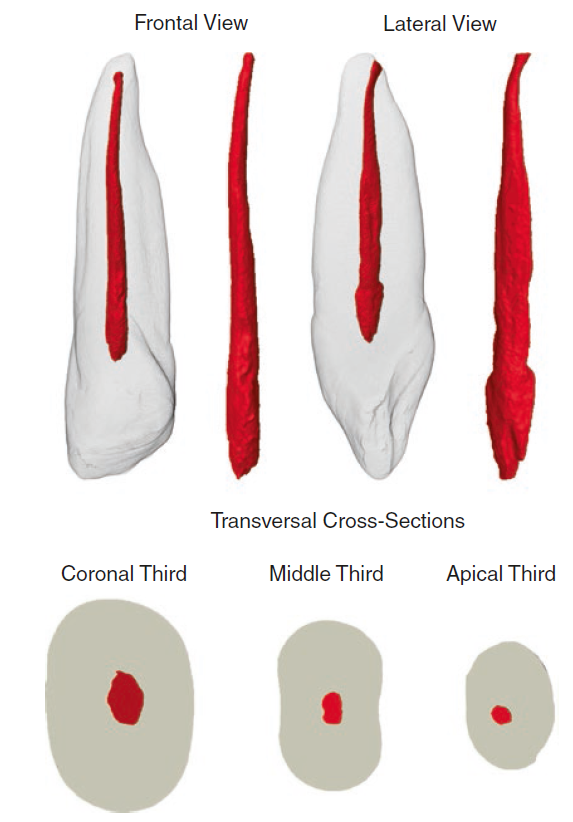
| Canal cross-section | Coronal, “egg-shaped” or ovoid; middle, oval; apical, round |
| Canal taper | BL, 0.08 mm/mm; MD, 0.04 mm/mm |
| Transverse anastomosis | – |
| Furcation canals | – |
| Apical foramen position | Central, 22%; lateral, 78% |
| Accessory canals | 5.5–26% (coronal, 1%; middle, 8%; apical, 91%) |
| Apical ramification | 3.9–23.6% |
| Canal curvature | Clinical view, 0–74°; proximal view, 0–55° |
| Canal diameter | BL: 0.45 mm (0.27–0.83 mm) MD: 0.33 mm (0.19–0.54 mm) |
| Anomalies | Two canals [21–23]; three canals [24, 25]; four canals [26]; two roots [27]; radicular groove [18]; fusion/gemination [28]; dens invaginatus [29]; dens evaginatus [30]; C-shaped canal [31]; talon cusp [32]; abrupt apical curvature [33] |
| Clinical remarks | This tooth often has anomalies and presents a high frequency of apical root curvature to the distopalatal direction; the lingual shoulder must be removed as it prevents direct access to the root canal and often results in ledge or perforation; the root canal is generally oval-shaped, and the root is frequently bent either buccally or distally; therefore, on the radiograph, the canal may appear shorter than it actually is |
the access cavity is created in the same way as in the central incisor. The pulp horns are often closely situated or singular in this tooth, resulting in a final shape that is more likely to be ovoid as opposed to triangular. Care must be taken when negotiating the apical curvature in this tooth, particularly with larger file sizes, which can result in canal transportation or ledging if not correctly identified